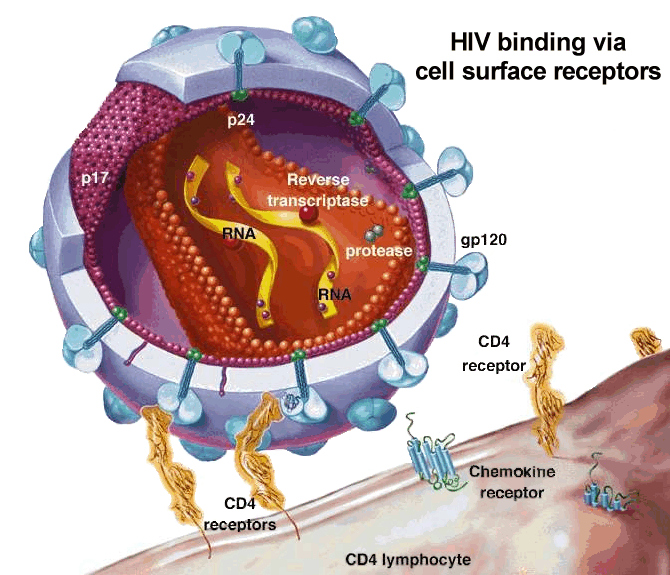
Retrovirus that targets and destroys CD4+ cells
CD 4+ count indicates degree of immunosuppression
History / PE:
Isolated thrombocytopenia (initial HIV presentation in 10%)
Mononuclosis-like or flu-like symptoms
Opportunistic infections
Nights sweats, weight loss
Diagnosis:
ELISA (high sensitivity, rule out HIV diagnosis)
Western blot (high specificity, confirmatory)
Rapid HIV tests
Treatment:
Initial regimen of two nucleoside/nucleotide reverse transcriptase inhibitors (RTIs) plus either one non-nucleoside RTI (NNRTI) or one protease inhibitor ( HIV therapy )
Use HIV polymerase chain reaction (PCR) to monitor the effectiveness of antiretroviral therapy (measures viral load)
CD4+ < 500, initiate HAART
CD4+ < 200, Bactrim prophylaxis for PCP
CD4+ < 75, Azithromycin prophylaxis for MAC
CD4+ < 50, Fluconazole prophylaxis for fungi
Pneumonic:
"The Major Pathogens Concerning Complete T-Cell Collapse"
Toxoplasma Gondii
M ycobacterium avium-intracellulare
P neumocystis jioveci
C andida albicans
Cryptococcus neoformans
T uberculosis
C MV
C ryptosporidium parvum (chronic diarrhea)
Notes:
1) Homozygous CCR5 mutation may confer resistance to HIV infection
2) MMR is the ONLY live vaccine to give to HIV patients
3) Do NOT give oral polio vaccine to HIV + pts or their contacts
4) MCC of pneumonia in HIV patients is Pneumococcus